Resolving the Fat Finger
![]()
March 2018 No. 49
Resolving the Fat Finger
by Judy Colditz OT/L, CHT, FAOTA
The internal resistance created by significant edema within the digit (the “fat finger”) impedes interphalangeal (IP) joint motion and favors easy movement at the metacarpophalangeal (MP) joint (See Figure 1).

Figure 1
Why is it sometimes so difficult to reduce a fat finger? Unlike other parts of the hand/arm where adjacent muscle contraction facilitates lymphatic flow, the absence of muscles within the finger means edema reduction is dependent on external treatment. Two common treatment approaches are compression and active motion.
Compression
The principle of compression to facilitate lymphatic flow is well known, but many—especially patients—think that if a little is good, a lot is better. Almost all compression wraps are applied too tightly around the finger and are bulky, thus actually impeding flexion (Gloves used for hand edema can also be too tight).
Stretchy self-adherent wrap is frequently used to apply compression to the finger, but it is almost impossible for a patient to wrap it loosely enough with one hand. A suggested alternative is the use of wide self-adherent wrap (width equal to the length of the finger); have the patient pinch the wrap together along one side of the finger and around the end (See Figures 2A-D). The goal is to apply the wrap as loosely as possible around the finger, applying equal light pressure to the skin. It is desirable that the wrap move slightly on the finger to allow easier motion.

Figure 2A: Patient pinches the wrap together on the sides and end of the finger assuring gentle tension on the wrap.

Figure 2B: Excess wrap is cut off leaving small flap of wrap material.

Figure 2C: Small flap is pressed down to finish seam.

Figure 2D: Finished wrap (on partially amputated finger).
Movement
Wrapping alone does not usually resolve finger edema unless accompanied by active interphalangeal joint motion.
Motion at the joints compresses the soft tissues and creates a “pumping” mechanism for lymphatic drainage.
Stiffness of the hand also includes multiple stiff, edematous fat fingers. Whether reducing an isolated edematous finger or edematous fingers that are part of a stiff hand, it is useful to focus on enabling lymphatic flow from the distal to the proximal portion of the hand. This requires interphalangeal joint motion to first pump the edema from the fingers.
Since stiff fingers always have an element of interosseous muscle tightness, the logical starting point is to first block the MP joints in extension (the position of interosseous muscle elongation). Interphalangeal joint tightness and edema may be resolved with a blocking exercise, but in the significantly stiff hand a non-removable cast is the best choice (See Figure 3).

Figure 3: Plaster of Paris cast directs motion to interphalangeal joints while providing contoured pressure to palm.
The cast prevents wrist and MP joint motion, assuring extrinsic flexor power is delivered across the stiff IP joints. It is important that the intimate fit of the cast provides consistent but non-restrictive pressure to the lymphatic network in the palm of the hand (See Figure 4).
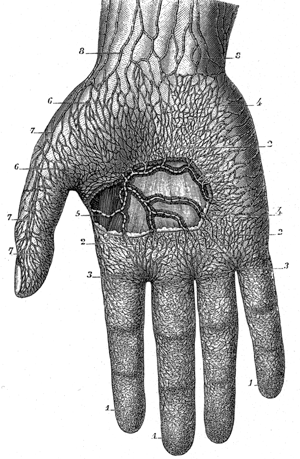
Figure 4: The palmar lymphatics as drawn by Sappey, 1876.
The cast must be molded precisely to provide both well contoured pressure to the palm and to adequately block the MP joints without blocking IP joint motion. Each time the fingers are flexed this network receives gentle compression, facilitating lymphatic flow.
Download Clinical Pearl No. 49, Resolving the Fat Finger, March 2018
© HandLab; 2018 all rights reserved
Disclaimer: HandLab Clinical Pearls are intended to be an informal sharing of practical clinical ideas; not formal evidence-based conclusions of fact.