Mallet Finger: A Change in Perspective
![]()
April 2023 No. 78
Mallet Finger: A Change in Perspective
by Karol S. Young OTD, OTR/L, CHT
A review of closed bony or tendinous mallet finger treatment reveals the accepted approaches are typically the same: fabricate an orthosis to immobilize the distal interphalangeal (DIP) joint in neutral to slight hyperextension continuously for 6 to 8 weeks. A recent article by Giddins, however, suggests that all mallet injuries are not equal and, therefore, should be treated differently.
Clinical Presentation: Tendinous Mallet Finger
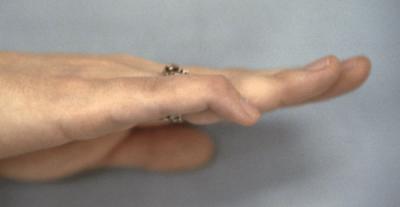
Patients with closed tendinous mallet finger injuries usually sustain these injuries during normal daily activities when the DIP joint is forced into flexion while holding the finger extended (Examples: holding the fingers extended to clean in the corner of a microwave or hitting a hard object while holding the fingers extended while cleaning a countertop.)
Forced hyperflexion of the DIP joint while the finger is extended ruptures the terminal tendon insertion of the dorsal apparatus. An insignificant piece of bone may be pulled off at the tendon insertion (bony avulsion) when this injury occurs.
These injuries are not painful and often the patient does not even remember the mechanism of injury. The mean age for individuals who experience a tendinous mallet finger injury is 57 years and involvement of multiple digits is rare.
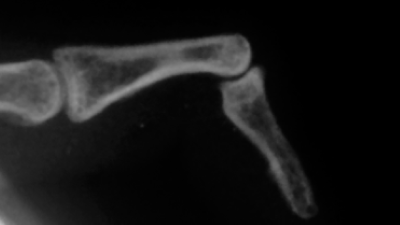
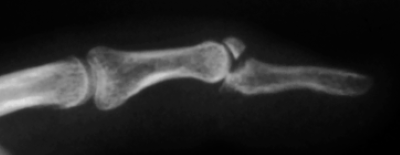
Example X-RAY of Tendinous Mallet Finger
Clinical Presentation: Bony Mallet Finger
A closed bony mallet injury results from a more forceful injury such as a fall, playing sports, or the result of trauma. These injuries occur most frequently in younger patients with the mean age of 40.
Unlike the tendinous mallet injury, bony mallet injuries often result from a forced hyperextension of the finger DIP joint.
Unlike the tendinous mallet injury, bony mallet injuries often result from a forced hyperextension of the finger DIP joint.
Example X-RAY of Bony Mallet Finger
The resulting fracture of the dorsum of the distal phalanx base may include significant articular involvement. The extensor tendon, however, stays intact as it remains connected to the bony fragment. The hyperextension DIP joint injury may also rupture the palmar aspect of the DIP joint capsule, which effects joint stability.
Bony mallet finger injuries are more painful than tendinous mallet finger injuries and may occur in more than one digit.
Type of Injury Determines Treatment
Tendon injuries in the hand take longer to heal than injuries to the bone because the tendon is relatively avascular. For a tendon to heal, the ends must be approximated without tension while fracture healing relies on bony alignment.
Using lateral x-rays to determine the DIP joint position, Giddens found that the extensor lag resulting from a tendinous mallet finger injury is greater than the lag created by a bony mallet injury.
Tendons require longer to heal than bone. The fact that tendinous injuries are more commonly seen in older patients with lessened tissue integrity means that the time required for healing in this group is always longer than younger patients who sustain a bony mallet injury.
Defining the two types of mallet injuries determines our treatment approach. See infographic.
- A tendinous mallet requires positioning the DIP joint in slight extension for 6-8 weeks to ensure tendinous healing.
- A bony mallet requires immobilization in neutral to slight flexion for 4 to 6 weeks to ensure bony alignment and reduce distal phalanx subluxation.

Mallet Finger Infographic (Click to download)
Our clinic provides this infographic above to newer therapists to guide them in determining the treatment plan for mallet finger injuries as well as to assist with clinical reasoning when the physician’s order does not differentiate between a tendinous or bony mallet.
Comparing the physical characteristics of the closed bony mallet finger injury versus tendinous mallet finger injury challenges us to think more critically about mallet finger treatment. Consider that all mallet finger injuries are not created equally and therefore should be treated the differently.