Nuances of Interosseous Muscle Tightness Testing
![]()
September 2012 No. 21
Nuances of Interosseous Muscle Tightness Testing
Judy Colditz, OT/L, CHT, FAOTA
The Normal Hand
Interosseous muscles are found on each side of most of the fingers, but we are not able to equally move each finger toward the radial and ulnar directions. We normally have considerably greater ulnar deviation than radial deviation at the MP joints. That means that the interosseous muscles that lie on the radial side of each finger (1st and 2nd dorsal & 2nd and 3rd volar interosseous) can be elongated more than the ones on the ulnar side (3rd & 4th dorsal and 1st volar interosseous). Additionally, common tasks such as cutting with a large knife or holding a tennis racket involve some element of ulnar deviation. Ulnar deviation in all fingers can often be found in individuals with rheumatoid arthritis and individual finger deviation can be seen following direct trauma to the palm (often a metacarpal fracture or stab wound).
In Clinical Pearls 19 & 20 we stated that the MP joint must be maintained in neutral alignment when hyperextended to accurately evaluate interosseous muscle tightness. With neutral alignment the interosseous muscles on both sides of the finger are equally tested. To test the radial and the ulnar sided interosseous muscles separately is more challenging because the normal difference of radial versus ulnar tightness must be considered.
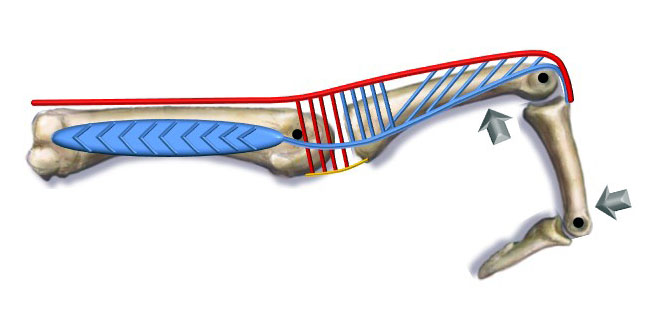
Position for testing interosseous muscle tightness
In most individuals, when the MP joint is held in maximum hyperextension and neutral alignment and the PIP joint in maximum flexion, it is impossible to maintain those joint positions and radially deviate the MP joint to any significant extent. The extent of deviation possible, however, becomes somewhat greater as one moves from the radial fingers to the ulnar fingers. When doing the same maneuver and ulnarly deviating the MP joint, the range of deviation is significantly greater in all fingers.
How Far Do I Take The MP Joint Into Hyperextension When There Is Bilateral Involvement
Many patients with bilateral involvement will not have an uninvolved hand to allow the examiner to establish that individual’s “normal.”
If this is the case, it will be impossible to determine the accurate maximum position for MP hyperextension. In my clinical experience it is extremely rare that a normal uninvolved finger cannot have the MP joint at least taken to 0° and most individuals will have some hyperextension when the PIP joint is also held in maximum flexion. I look at the patient’s other MP joints to determine if they display an element of hyperextension. If they do, I position the MP joint in a maximum of 20 degrees hyperextension for the testing; if not, I only
I look at the patient’s other MP joints to determine if they display an element of hyperextension. If they do, I position the MP joint in a maximum of 20 degrees hyperextension for the testing; if not, I only take the MP joint to neutral. Although there is no assurance of accuracy in this approach, the first testing establishes a baseline score from which one may observe progress or lack of progress. To accurately document change, it is important that all subsequent MP joint testing positions are identical to the first.
Ulnar Versus Radial Interosseous Tightness Testing
When testing for ulnar versus radial interosseous tightness, the normal difference in radial versus ulnar sided interosseous tightness must be considered. In patients with bilateral involvement it seems reasonable that the MP joint while hyperextended with the PIP joint maximally flexed, should at least be taken to 0 degrees in the radial direction, increasing perhaps to 10 degrees in the ring and little fingers. One may conversely expect ulnar deviation at the MP joint to be greater, at least 10-20 degrees.
Step 1 - Ulnar-Sided Interosseous Testing (Radial Deviation):
1. Position the MP joint in neutral to 10° radial deviation (see above) and then passively hyperextend the MP joint. [If you are unable to evaluate the normal contralateral finger to know how far to hyperextend the MP joint, it is reasonable to take it to 10-20°, but each subsequent exam must repeat the same position of MP hyperextension so accurate comparisons can be made.
2. Maintain this position of the MP joint while passively flexing the PIP to its easy maximum.
3. With both joints positioned, measure the angle of MP joint hyperextension and the angle of PIP joint flexion and add them together. Note the alignment position of the MP joint when the score is taken.
Step 2 - Radial-Sided Interosseous Testing (Ulnar Deviation):
1. Position the MP joint in easy maximum ulnar deviation (see above) and then passively hyperextend the MP joint. [If you are unable to evaluate the normal contralateral finger to know how far to hyperextend the MP joint, it is reasonable to take it to 10-20°, but each subsequent exam must repeat the same position of MP hyperextension so accurate comparisons can be made.
2. Maintain this position of the MP joint while passively flexing the PIP to its easy maximum.
3. With both joints positioned, measure the angle of MP joint hyperextension and the angle of PIP joint flexion and add them together. Note the alignment position of the MP joint when the score is taken.
Additional Suggested Reading
Clinical Pearl No. 33 – How Can Each Therapy Visit be as Focused and Productive as Possible?
Clinical Pearl No. 27 – Complex Made Simple: Pasta Transfer
Clinical Pearl No. 22 – Lumbrical Muscle Tightness & Testing
Clinical Pearl No. 21 – Nuances of Interosseous Muscle Tightness Testing
Clinical Pearl No. 20 – Quantifying Interosseous Muscle Tightness
Clinical Pearl No. 19 – Interosseous Muscle Tightness Testing
Clinical Pearl No. 3 – Making the Most of Mallet Finger Splinting
Download Clinical Pearl No. 21, Nuances of Interosseous Muscle Tightness Testing, September 2012
© BraceLab; 2014 all rights reserved
Disclaimer: BraceLab Clinical Pearls are intended to be an informal sharing of practical clinical ideas; not formal evidence-based conclusions of fact.