Quantifying Interosseous Muscle Tightness Testing
![]()
July 2012 No. 20
Quantifying Interosseous Muscle Tightness Testing
Judy Colditz, OT/L, CHT, FAOTA
In our last Clinical Pearl, we discussed interosseous muscle testing and this Clinical Pearl continues the discussion. Please review the last HandLab Clinical Pearl No.19 before reading below.
Treatment to reduce stiffness of a finger must be goal oriented and evaluation measurements must quantify progress toward the goal. Resolving interosseous muscle tightness is usually one of the early steps in regaining full motion and function of the digit but has remained a vague and unquantifiable goal. Below is a procedure for quantifying interosseous muscle tightness which precisely defines the goal and allows measurement toward the goal. First test to see if interosseous tightness is present in the injured/involved finger (see HandLab Clinical Pearl No.19). If the answer is yes, proceed to quantifying.
Step 1: Test for normal interosseous muscle length on uninjured/uninvolved contralateral finger:
1. Passively extend the MP joint (with the MP joint in neutral alignment) to its easy maximum while maintaining full passive PIP joint flexion.
2. Measure the angle of MP joint hyperextension and the angle of PIP joint flexion.
3. Add these numbers together to obtain the normal interosseous muscle elasticity score for that finger. This number equals 100% of normal interosseous muscle elasticity for that finger.
Step 2: Test for Interosseous muscle length on the injured/involved finger:
1. Passively extend the MP joint (with the MP joint in neutral alignment) to, but not beyond, the angle of MP joint hyperextension measured on the contralateral finger.
2. Maintain this position of the MP joint while passively flexing the PIP joint to its easy maximum.
3. With both joints positioned, measure the angle of MP joint hyperextension and the angle of PIP joint flexion and add them together. This number equals the interosseous muscle elasticity of this finger. (If the MP joint will not extend to 0°, it is a negative number which is subtracted.)
Step 3: Determine the interosseous muscle tightness score:
Divide the score from Step 2 (injured finger) by the score from Step 1 (the normal uninjured finger) to calculate the percentage of normal interosseous muscle elasticity in the injured finger.
Consider these examples:
Example 1:
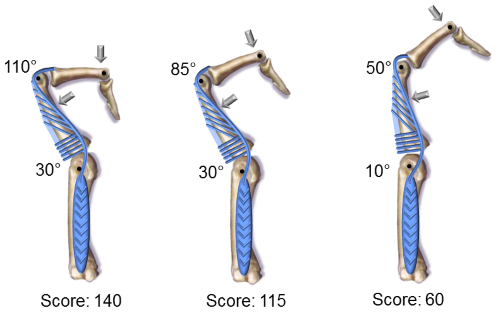
Patient’s normal uninjured long finger passively hyperextends at the MP joint to 30 degrees while the PIP joint is held at 110 degrees. Adding these two numbers together gives the normal interosseous muscle elasticity score of 140, which equals 100% (See NORMAL illustration below).
• The PIP joint of the patient’s injured finger can be flexed only to 85 degrees when the MP joint is held at 30 degrees hyperextension (see EXAMPLE 1 illustration below). These two numbers added together gives the abnormal interosseous muscle elasticity score of 115.
• Since 115 is less than 140, there is less than normal interosseous muscle elasticity in this finger. By dividing 140 into 115 we determine that the injured finger has 82% of normal interosseus muscle elasticity (or an 18% reduction).
Example 2:
Imagine that the injured finger has very limited passive PIP joint flexion as well as limited passive MP joint extension (not unusual in a stiff finger).
• The uninjured finger is the same as above with a score of 140.
• The injured finger will only passively flex at the PIP joint to 60 degrees and the MP joint will only hyperextend 10 degrees.
• The first question is whether there is LESS passive PIP joint flexion with the MP joint extended than with it flexed. If the answer is yes, scoring is appropriate.
• When the MP joint is hyperextended to 10 degrees, the PIP joint will only flex to 50 degrees (less than when the MP joint was flexed). See EXAMPLE 2 above. Adding these numbers together, the score for in the injured finger is 60 or 43% of normal interosseus elasticity (or a 57% reduction).
With this scoring system, serial examinations allow documentation of progress (or lack of) in reducing interosseous muscle tightness.
Additional Suggested Reading
Clinical Pearl No. 33 – How Can Each Therapy Visit be as Focused and Productive as Possible?
Clinical Pearl No. 27 – Complex Made Simple: Pasta Transfer
Clinical Pearl No. 22 – Lumbrical Muscle Tightness & Testing
Clinical Pearl No. 21 – Nuances of Interosseous Muscle Tightness Testing
Clinical Pearl No. 20 – Quantifying Interosseous Muscle Tightness
Clinical Pearl No. 19 – Interosseous Muscle Tightness Testing
Clinical Pearl No. 3 – Making the Most of Mallet Finger Splinting
Download Clinical Pearl No. 20, Quantifying Interosseous Muscle Tightness Testing, July 2012
© BraceLab; 2014 all rights reserved
Disclaimer: BraceLab Clinical Pearls are intended to be an informal sharing of practical clinical ideas; not formal evidence-based conclusions of fact.